


Update: Our papers presenting an independent analysis of Dr. Didier Raoult's data, with stunning results, have now been published
By Eleftherios Gkioulekas, PhD

I am pleased to announce the publication of two major refereed research papers [1,2] in which we reported the results of an independent analysis of the data by Dr. Didier Raoult and colleagues on 30,423 COVID-19 patients treated in IHU Mediterranean in Marseilles, France through December 2021 [3]. The attached video is a short presentation by Professor Christian Perronne to the 2024 International Crisis Summit, in which he announced the two papers. At that time, both papers had already been accepted for publication.
[continued below the video and graphical abstracts]

Background
Prof. Christian Perrone, the senior author of both papers, assembled an interdisciplinary team that included Dr. Valere Lounnas, Prof. Eleftherios Gkioulekas, Dr. Marc Rendell, Dr. Alexis Lacout, and Xavier Azalbert. The project was spearheaded by Dr. Valere Lounnas, the corresponding author of both papers. The team collaborated on this project over a period of 7 months, with extensive discussions on improving the computations, validating the statistical methodology with extensive sensitivity analysis, and organizing the presentation of the results in a methodical way in the two manuscripts. The first paper examines the efficacy of Dr. Raoult's early treatment protocol with respect to preventing the combined events of admission to the Intensive Care Unit (ICU) and/or death [1]. The second paper examines whether the primary series of COVID-19 vaccinations used in France had any beneficial effect towards preventing admission to the ICU and/or death [2]. News coverage of this work has already been reported by France Soir in two articles, for the first and second paper respectively.
Dr. Didier Raoult and his colleagues were forced to withdraw an early preprint showing the efficacy of their early treatment protocol, using the complete dataset of pre-omicron patients through December 2021, because of threats of professional reprisal, especially against their junior colleagues, by certain elements from both the French government and French academia, amplified by some news media outlets. In response to these threats, Dr. Raoult and colleagues, for the first time, published their complete raw data set [3], to enable scientists from all around the world to analyze it independently. Our group began work shortly after the publication of Dr. Raoult's data. While our work was in progress, a study was published by the senior leaders of Dr. Raoult's group in collaboration with Dr. Peter McCullough, which examined the efficacy of the early treatment protocol based on the published data [4]. Our independent analysis has confirmed and extended their work.
The threats against Dr. Raoult's group that occurred during 2023 and 2024 are very puzzling, because a comprehensive analysis of their data through the end of December 2020 had already been published in the peer reviewed literature, showing that his early treatment protocol was efficacious in preventing the deaths of high-risk patients [5]. Furthermore, a case series statistical analysis technique was introduced and used to show that Dr. Vladimir Zelenko's data on his triple drug therapy of hydroxychloroquine, azithromycin, and zinc had established a clear and convincing finding of mortality rate reduction for high-risk patients by June 2020, and a clear and convincing finding of hospitalization rate reduction for high-risk patients by April 2020 [6], thus providing the needed mathematical foundation to vindicate the original assessment by Dr. Harvey Risch concerning the efficacy of Dr. Zelenko's triple drug therapy [7]. Therefore, it was clear as day at the beginning of May 2020 that there was sufficient evidence to justify the ethics of using the triple drug therapy in treating COVID-19 patients. With the publication of Raoult's analysis of his data through the end of December 2020 [5], there was sufficient evidence to support the efficacy of his treatment protocol. With the additional data through December 2021, what can be done now, that was not possible before, is to study the complex interactions between COVID-19 risk factors, treatment, and vaccination.
Finally, contrary to circulating disparaging claims, there was no unethical experimentation in the treatment of COVID-19 patients and Raoult and colleagues did not conduct a clinical trial. Patients were offered an experimental treatment option, when not contraindicated, in addition to standard of care, and the option was accepted or rejected by the patients with informed consent, as per Article 37 of the 2013 Helsinki declaration [8], the precise statement of which reads:
"In the treatment of an individual patient, where proven interventions do not exist or other known interventions have been ineffective, the physician, after seeking expert advice, with informed consent from the patient or a legally authorised representative, may use an unproven intervention if in the physician's judgement it offers hope of saving life, re-establishing health or alleviating suffering. This intervention should subsequently be made the object of research, designed to evaluate its safety and efficacy. In all cases, new information must be recorded and, where appropriate, made publicly available."
In the process of ethical patient treatment, real world data is generated and furthermore, Article 37 requires researching and disseminating the real world data resulting from any attempts at using an unproven treatment. Therefore, it is the threats of professional reprisal directed against Raoult and colleagues, to dissuade them from publishing their results in the peer-reviewed research literature, that constituted a blatant violation of medical ethics.
Part 1: Early treatment efficacy
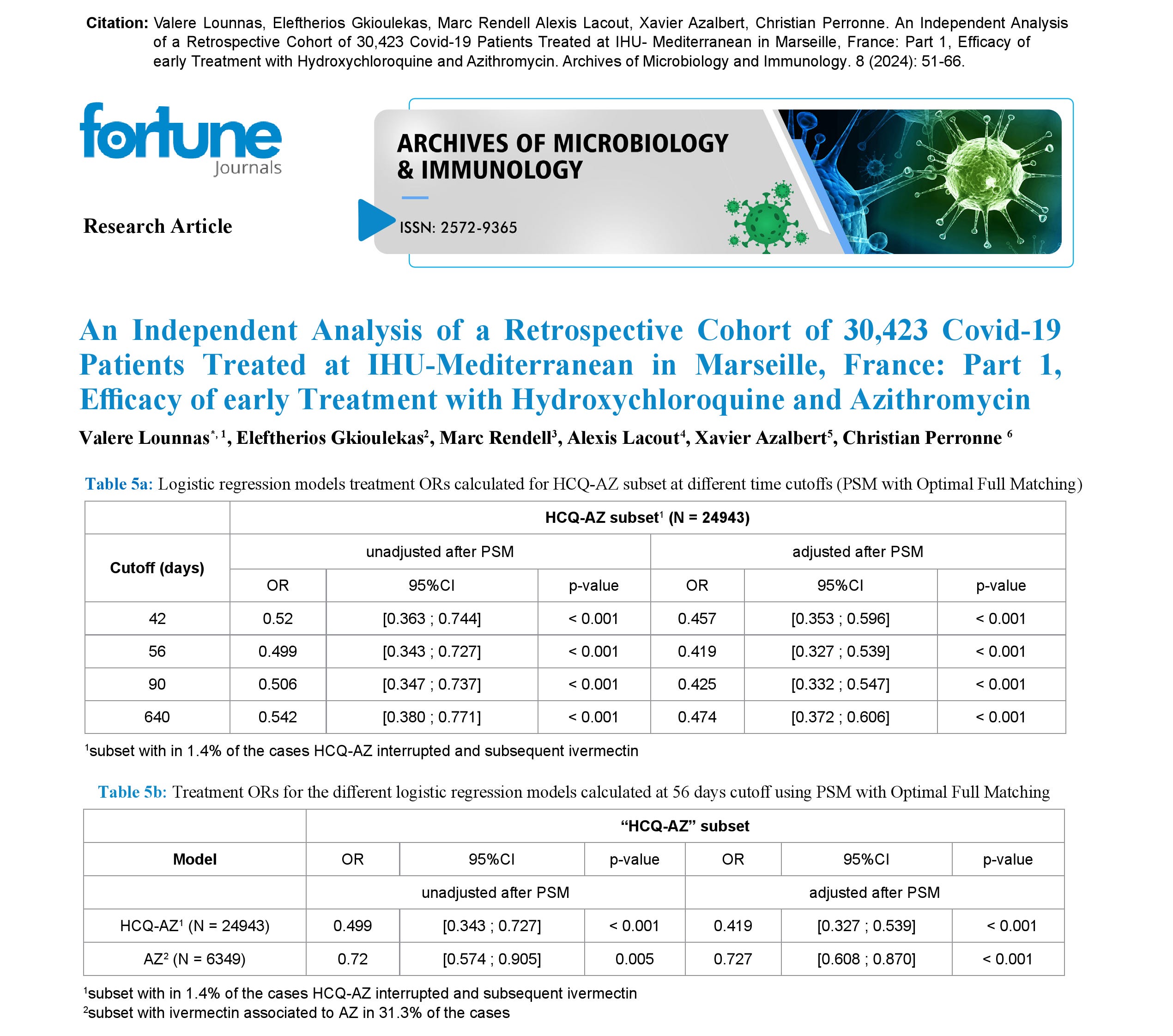
In Part 1 of our study [1], we used as treatment group the subset consisting of patients that received either the combination of hydroxychloroquine and azithromycin or azithromycin alone on an intent to treat basis (i.e. for some small proportion of patients the treatment may have been interrupted followed by subsequent ivermectin treatment). As control group we used the subset of patients that received no hydroxychloroquine, no azithromycin, and no ivermectin. Patients forming the control group did not receive these medications either due to not consenting to treatment or due to contraindications. Both groups received a standard of care that included zinc supplementation, enoxaparin for patients older than 70 or with comorbidities, and low-dose dexamethasone for patients with inflammatory pneumonopathy, high viral loads (necessitating frequent testing to monitor viral loads) or based on physician judgment on a case-by-case basis.
To compare the two groups, we used propensity score matching with optimal full matching to balance the covariates in both groups, thus simulating the randomization between the treatment and control group, usually achieved in the context of a randomized controlled trial, followed with logistic regression analysis. The comparison endpoint was the composite of admission to the Intensive Care Unit (ICU) and deaths within 42 days, 56 days, and 90 days. The corresponding adjusted odds ratios for the patients that received the combination of both hydroxychloroquine and azithromycin with standard of care were 0.457 (95% CI 0.353--0.596) within 42 days, 0.419 (95% CI 0.327--0.539) within 56 days, and 0.425 (95% CI 0.332--0.547) within 90 days. We note that there is an overall trend of improvement as the cutoff is extended from 42 days to 90 days. For patients that received only azithromycin with standard of care, using the 56 days cutoff, the corresponding adjusted odds ratio was 0.727 (95% CI 0.608--0.870). Thus, we have found that, with a 56 days cutoff, the combined hydroxychloroquine and azithromycin treatment has 58% efficacy and azithromycin alone has 27% efficacy in preventing the composite outcome of ICU admission and/or death. All of these results are statistically significant with p < 0.001.
Further analysis showed favorable interactions between combined hydroxychloroquine and azithromycin treatment and age categories greater than 49 years, patients with obesity, COPD, cancer, immunodeficiency, and male patients. This means that treatment is associated with a decrease in the adjusted risk attributed to all patient characteristics that have been identified as risk factors for ICU admission and deaths. Equivalently, there are no subsets of high-risk patients for whom treatment could be contraindicated. There is no statistically significant interaction between the combined treatment and vaccination status, indicating that vaccination status does not impact the efficacy of the combined treatment. It is important to emphasize that the control group also received some standard of care treatment that was superior to what was recommended at the time by public health authorities. Therefore, the efficacy reported in our paper underestimates the true efficacy of Dr. Raoult's treatment protocols, when compared against the recommendations of public health authorities. One limitation of our analysis is that we do not know for each patient the time delay between symptomatic infection and initiation of treatment. It is biologically plausible that reduced time delay would contribute towards better efficacy.
Part 2: Vaccination efficacy
In part 2 of our study [2], we analyzed a subset of 16063 patients with known vaccination status between November 23, 2020, and December 21, 2021. A similar methodology of combining propensity score matching with optimal full matching and logistic regression analysis was used to compare the vaccinated group against the unvaccinated group in terms of the composite endpoint of admission to ICU or death using 42 days, 56 days, and 90 days as cutoffs for counting adverse events. At the 42-day cutoff we found an adjusted odds ratio of 0.438 (95% CI 0.307--0.670), corresponding to 56% efficacy in reducing admissions to the ICU and/or deaths. Unlike the trend observed with early treatment, extending the cutoff to 56 days and 90 days shows a trend of decreasing efficacy with odds ratio 0.462 (95% CI 0.307--0.670) at 56 days and 0.486 (95% 0.326--0.700) at 90 days, corresponding to 53% efficacy at 56 days and 51% efficacy at 90 days. This decreasing trend could be a signal of a long-term adverse effect of vaccination, but it could also reflect some bias, not adjusted for by our analysis, that healthier patients are less likely to accept vaccination. Statistically significant favorable interaction was found between vaccination and delta variant. Favorable interactions with only borderline significance were also indicated between vaccination and obesity (p=0.084) and between vaccination and chronic cardiovascular comorbidities (p=0.090). However, statistically significant unfavorable interactions were found between vaccination and severity of disease (indicated by inpatient admission), age > 89 years, and immunodeficiency. An unfavorable interaction with borderline significance was also indicated between vaccination and COPD (p=0.072). Unfavorable interactions signal decreased efficacy in preventing ICU admissions and/or deaths in the respective subgroups. Equivalently, unfavorable interactions between vaccination and specific risk factors suggest an exacerbation of the adjusted risk attributed to these risk factors as a consequence of vaccination. Furthermore, subgroup analysis of the age < 50 years subset showed no efficacy of vaccination in preventing ICU admissions and/or deaths.
Putting the results in context
To put these results in context, we should also mention that a meta-analysis [9] of the hydroxychloroquine pre-exposure prophylaxis protocol, recommended by the Indian Council of Medical Research [10], demonstrated at least 75% efficacy in preventing COVID-19 infection in healthcare workers. Combining the 75% efficacy of the prophylactic protocol with the 58% efficacy of the treatment protocol results at least in an overall 89% efficacy in overall risk reduction for ICU admission or deaths from the combined effect of reducing infections and reducing ICU admissions and/or deaths, if infected. This is a lower bound, since we are expecting a favorable interaction between prophylaxis and treatment in which prophylaxis should intensify the efficacy of the risk reduction attributable to the treatment. Obviously, this was an option that was always on the table as early as March 2020, recommended both by the late Dr. Vladimir Zelenko and the ICMR, for which we had sufficient supporting evidence as early as May 2020, whereas we had to wait until the beginning of 2021 for the vaccine roll-out.
However, to fully understand the context of our reported results the following additional considerations also have to be taken into account:
1. Vaccines are relevant to public health if they provide permanent sterilizing immunity that cuts the chain of transmission. The mere existence of vaccinated patients in Dr. Raoult's dataset shows that vaccinated patients can also be infected, and presumably transmit the virus. Therefore, there is no public health interest in mandating vaccinations and in instituting systems such as vaccine passports for the COVID-19 vaccines. The existence of any personal benefit in and of itself is not sufficient to justify widely adopted vaccine mandate policies that violated, through coercion and threats of reprisal, the principles of informed consent.
2. It is well known at this time that the COVID-19 vaccines themselves can be responsible for serious adverse events that include admission to the ICU and death [11,12]. The cause of these adverse events can be attributed to the use of the SARS-CoV-2 spike protein as the vaccine antigen [13,14]. Furthermore, there are additional concerns specifically with the safety of the mRNA platform itself [15,16]. The risk for vaccine injury is further exacerbated by the persistence of spike protein in the human body for a period of at least 15 months [17], resulting in the bioaccumulation of spike protein with repeated vaccinations in conjunction with breakthrough COVID-19 infections. These adverse events are not captured by the Raoult dataset, which includes only patients that have not yet died by an adverse reaction to the COVID-19 vaccine. For these patients, there seems to be a consolation prize: the antiviral effect of vaccine induced antibodies by the primary vaccine series against the pre-omicron COVID-19 variants, on average, provided more benefit than the harm from the combined accumulation of spike protein from both the vaccine and the COVID-19 infection. It is not possible to calculate, from Raoult's database alone, whether the combination of ICU admissions and/or deaths, prevented by the COVID-19 vaccines, outweigh the ICU admissions and deaths caused by vaccination. However, both need to be taken into account to correctly calculate the true magnitude of vaccine efficacy. As it stands, our odds ratio overestimates the true vaccine efficacy by an unknown and uncontrolled margin.
In light of the above, the most important finding of our work is that it demonstrates the existence of counterbalanced harms and benefits both caused by the COVID-19 vaccination. This can be seen by the unfavorable interactions between vaccination and immunocompromised status, age > 89, and COPD. For both immunocompromised patients and frail nonagenarian patients where one expects diminished antiviral response induced by vaccination, the counterbalance between harm and benefit shifts towards harm. We see a similar unfavorable interaction in COPD patients, due to the increased harm caused by excess spike protein in frail lungs, which is known to precipitate oxygen desaturation leading to death [18]. We also see that the risk of ICU admissions and/or deaths is exacerbated in patients with more severe COVID-19, which can be explained by the excess accumulation of spike protein from both the prior vaccination and the subsequent infection.
What it all means
We already knew, before even beginning this study, that the early outpatient treatment protocol used by Raoult and colleagues was efficacious. We also knew that prophylactic use of hydroxychloroquine had 75% efficacy in preventing COVID-19 infection, which was comparable to the claimed corresponding efficacy of the COVID-19 vaccines in reducing infections. Separately from everyone that was injured or died from adverse events caused by vaccination, a much larger number of people were injured or died from denial of early outpatient treatment and denial of the prophylactic use of hydroxychloroquine. All of this is old news.
In plain English, what we have learned from this study is the following. First, we have found no vaccine efficacy for the age < 50 demographic, for whom vaccination presents only opportunity for harm. Beyond that, we have shown that vaccination exacerbates the risk presented by certain comorbidities, and it is therefore clearly contraindicated for these groups. Because one of these groups is patients that came down with severe COVID-19, it becomes impossible to reliably identify all patients for whom the vaccines are contraindicated, making it impossible to identify the group of patients for whom there could be some unclear theoretical net benefit.
Our results are consistent with the biologically plausible expectation that, by relying on the toxic spike protein for an antigen, COVID-19 vaccination will result in counterbalanced benefit, from the antiviral mechanism of vaccine-induced antibodies, and harm, from the toxicity and bioaccumulation of the SARS-CoV-2 spike protein. As the virus mutates, in part due to selective pressure from the widespread deployment of COVID-19 vaccinations that fail to provide sterilizing immunity, the anti-viral benefit will decrease, and over time this will shift the counterbalance between benefit and harm towards harm, resulting in negative efficacy. As vaccine boosters are administered every 6 months, the harm will increase monotonically with increasing spike protein accumulation and inevitably overtake any oscillating benefit from any transient antiviral effect from each booster administration. So, from a long-term perspective, the repeating vaccination strategy has no path to success.
With the prospect of permanent sterilizing protection via vaccination off the table, efforts should have been redirected towards early treatment, which has been shown by our studies to provide an equivalent or better benefit more safely, and other interventions such as using hydroxychloroquine prophylactically to provide additional protection to high-risk patients, and a pivot to the prophylactic use of monoclonal antibodies for immunocompromised and very frail patients. Chemoprophylaxis would then substitute for the temporary anti-infective action of COVID-19 vaccination and early treatment would substitute for the antiviral action of vaccine-induced antibodies in case of a symptomatic infection. Although these prophylactic alternative options can only provide temporary protection, in combination with early outpatient treatment, they add up towards a strategy of minimizing the total exposure to the SARS-CoV-2 spike protein and would have therefore minimized overall long-term harm. This strategy should have certainly been pursued, when the failure of the primary vaccine series became apparent, in lieu of pursuing vaccine boosters.
Some would argue that the prevalence of severe adverse events, reported in passive pharmacovigilance systems, during the first few months of the primary series vaccine rollout, were sufficient justification for suspending the vaccination strategy. With safer successful alternatives to the failing and unsafe vaccination strategy at hand, any continuation of COVID-19 vaccination at this time would be a clear violation of the Hippocratic Oath.
References
[1] V. Lounnas, E. Gkioulekas, M. Rendell, A. Lacout, X. Azalbert, C. Perronne, "An independent analysis of a retrospective cohort of 30,423 Covid-19 patients treated at IHU-Mediterranean in Marseille, France: Part 1, Efficacy of early treatment with hydroxychloroquine and azithromycin", Archives of Microbiology and Immunology 8 (2024), 51-66
[2] V. Lounnas, E. Gkioulekas, M. Rendell, A. Lacout, X. Azalbert, C. Perronne, "An independent analysis of a retrospective cohort of 30,423 Covid-19 patients treated at IHU-Mediterranean in Marseille, France: Part 2, A real-life assessment of Covid-19 vaccination efficacy", Archives of Microbiology and Immunology 8 (2024), 67-83
[3] P. Brouqui P, D. Raoult. "Construction, quality control and regulatory aspect of a database of 30,423 COVID-19 patients cared for at the IHU Méditerranée infection France", Biomedical Journal of Scientific & Technical Research 52(3) (2023), 43799-43804
[4] P. Brouqui, M. Million, P. Parola, P.A. McCullough, D. Raoult. "Outcomes after early treatment with hydroxychloroquine and azithromycin: An analysis of a database of 30,423 COVID-19 patients", New Microbes and New Infections 55 (2023), 101188
[5] M. Million, J-C. Lagier, H. Tissot-DuPont, I. Ravaux, C. Dhiver, C. Tomei, N Cassir, L. DeLorme, S. Cortaredona, S. Gentile, E. Jouve, A. Giraud-Gatineau, H. Chaudet, L. Camoin-Jau, P. Colson, P. Gautret, P-E. Fournier, B. Maille, J-C. Deharo, P. Habert, J-Y. Gaubert, A. Jacquier, S. Honore, K. Guillon-Lorvellec, Y. Obadia, P. Parola, P. Brouqui, D. Raoult, IHU COVID-19 Task Force. "Early Treatment with Hydroxychloroquine and Azithromycin in 10,429 COVID-19 Outpatients: A Monocentric Retrospective Cohort Study", Reviews in Cardiovascular Medicine 22 (2021), 1063-1072
[6] E. Gkioulekas, P.A. McCullough, V. Zelenko: "Statistical analysis methods applied to early outpatient COVID-19 treatment case series data", COVID 2(8) (2022), 1139-1182
[7] H.A. Risch. "Early Outpatient Treatment of Symptomatic, High-Risk Covid-19 Patients that Should be Ramped-Up Immediately as Key to the Pandemic Crisis", American Journal of Epidemiology 189 (2020), 1218-1226
[8] World Medical Association. "World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects", JAMA 310(20) (2013), 2191-2194.
[9] R.B. Stricker and M.C. Fesler. "Hydroxychloroquine Pre-Exposure Prophylaxis for COVID-19 in Healthcare Workers from India: A Meta-Analysis", Journal of Infection and Public Health 14 (2021), 1161-1163
[10] Indian Council of Medical Research, "Revised advisory on the use of Hydroxychloroquine (HCQ) as prophylaxis for SARS-CoV-2 infection (in supersession of previous advisory dated 23rd March, 2020)", 2020. Available at https://www.icmr.gov.in/pdf/covid/techdoc/V5_Revised_advisory_on_the_use_of_HCQ_SARS_CoV2_infection.pdf (accessed on January 9, 2024)
[11] J. Rose, "A report on the US Vaccine Adverse Events Reporting System (VAERS) of the COVID-19 messenger ribonucleic acid (mRNA) biologicals", Science, Public Health Policy, and the Law 2 (2021), 59-80.
[12] J. Rose, "Critical appraisal of VAERS Pharmacovigilance: Is the U.S. Vaccine Adverse Events Reporting System (VAERS) a functioning pharmacovigilance system?", Science, Public Health Policy, and the Law 3 (2021), 100-129
[13] P.I. Parry, A. Lefringhausen, C. Turni, C.J. Neil, R. Cosford, N.J. Hudson, J. Gillespie, "'Spikeopathy': COVID-19 Spike Protein Is Pathogenic, from Both Virus and Vaccine mRNA", Biomedicines 11 (2023), 2287
[14] J.-F. Lesgards, D. Cerdan, C. Perronne, J.-M. Sabatier, X. Azalbert, E.A. Rodgers, P.A. McCullough, "Toxicity of SARS-CoV-2 Spike Protein from the Virus and Produced from COVID-19 mRNA or Adenoviral DNA Vaccines", Archives of Microbiology and Immunology 7 (2023), 121-138.
[15] M.T.J. Halma, J. Rose, T. Lawrie. "The Novelty of mRNA Viral Vaccines and Potential Harms: A Scoping Review", J -- Multidisciplinary Scientific Journal 6 (2023), 220-235.
[16] K. Acevedo-Whitehouse, R.Bruno, "Potential health risks of mRNA-based vaccine therapy: a hypothesis", Medical Hypotheses 171 (2023), 111015
[17] B.K. Patterson, E.B. Francisco, R. Yogendra, E. Long, A. Pise, H. Rodrigues, E. Hall, M. Herrera, P. Parikh, J. Guevara-Coto, T.J. Triche, P. Scott, S. Hekmati, D. Maglinte, X. Chang, R.A. Mora-Rodríguez, J. Mora. "Persistence of SARS CoV-2 S1 Protein in CD16+ Monocytes in Post-Acute Sequelae of COVID-19 (PASC) up to 15 Months Post-Infection", Frontiers in Immunology 12 (2022), 746021.
[18] D.E. Scheim, P. Vottero, A.D. Santin, A.G. Hirsh, "Sialylated Glycan Bindings from SARS-CoV-2 Spike Protein to Blood and Endothelial Cells Govern the Severe Morbidities of COVID-19", International Journal of Molecular Sciences 24 (2023), 17039.