

From his earliest interviews, as early as April 2020, Dr. Zelenko recommended the use of prophylactic hydroxychloroquine, taken once a week, combined with daily zinc sulfate, to prevent symptomatic COVID-19 infections. He first published his prophylactic protocol document during the Summer 2020, after surviving open heart surgery:
Zelenko Covid-19 Prophylaxis Protocol
Prophylaxis is an action taken to prevent or protect against a specified disease. Greek in origin, from the word "phylax", meaning "to guard" and "watching."
Low Risk Patients
Young healthy people do not need prophylaxis against Covid 19. In young and healthy people, this infection causes mild cold-like symptoms. It is advantageous for these patients to be exposed to Covid-19, build up their antibodies and have their immune system clear the virus. This will facilitate the development of herd immunity and help prevent future Covid-19 pandemics. However, if these patients desire prophylaxis against Covid-19, then they should take the protocol noted below.
Moderate Risk Patients
Patients from this category are healthy but have high potential viral-load exposure. This group includes medical personnel, caregivers of high-risk patients, people who use public transportation, first responders and other essential personnel who are crucial to the continued functioning of society. These patients should be encouraged to take prophylaxis against Covid-19 in accordance with the protocol noted below.
High Risk Patients
Patients are considered high risk if they are over the age of 45, or if they are younger than 45 but they have comorbidities, that is, they have other health conditions that put them at risk. These patients have between a 5 to 10% mortality rate if they are infected with Covid-19. These patients should be strongly encouraged to take prophylaxis against Covid-19 in accordance with the protocol noted below.
Protocol for Low and Moderate Risk Patients:
Elemental Zinc 25mg 1 time a day Vitamin D3 5000iu 1 time a day Vitamin C 1000mg 1 time a day Quercetin 500mg 1 time a day until a safe and efficacious vaccine becomes available. If Quercetin is unavailable, then use Epigallocatechin-gallate (EGCG) 400mg 1 time a day.
Protocol for High Risk Patients:
Elemental Zinc 25mg once a day Vitamin D3 5000iu 1 time a day Hydroxychloroquine (HCQ) 200mg 1 time a day for 5 days, then 1 time a week until a safe and efficacious vaccine becomes available. If HCQ is unavailable, then use the Protocol for Low and Moderate Risk Patients.
The rationale for the original hydroxychloroquine chemoprophylaxis protocol is that, zinc ions inhibit the replication of the SARS-CoV-2 virus by interfering with the function of the RNA RNA dependent RNA polymerase (RDRP) protein used by the virus to replicate. Hydroxychloroquine allows zinc to enter the cells. Dr. Zelenko used to explain this with a gun and a bullet analogy, where hydroxychloroquine functions as the gun and zinc functions as the bullet; it takes both to create a working system. Nevertheless, hydroxychloroquine, by itself, has additional mechanisms of action for preventing the virus from entering the cell in the first place. Both mechanisms are not specific to any particular strain of the virus, so the protection is broad-spectrum against all strains. The virus could only adapt by increasing its replication rate, thus lowering the threshold for the initial viral load sufficient to result in a breakthrough infection, however a geometric increase in the replication rate can only result in an approximately linear decrease of the window of opportunity for treating a symptomatic infection.
An updated prophylactic protocol was later announced by Dr. Zelenko on February 2021, which included the option of using ivermectin prophylactically:
Zelenko Covid-19 Prophylaxis Protocol
Website: Vladimirzelenkomd.com
Prophylaxis is an action taken to prevent or protect against a specified disease. Greek in origin, from the word "phylax", meaning "to guard" and "watching."
Low Risk Patients
Young healthy people do not need prophylaxis against Covid 19. In young and healthy people, this infection causes mild cold-like symptoms. It is advantageous for these patients to be exposed to Covid-19, build up their antibodies and have their immune system clear the virus. This will facilitate the development of herd immunity and help prevent future Covid-19 pandemics. However, if these patients desire prophylaxis against Covid-19, then they should take the protocol noted below.
Moderate Risk Patients
Patients from this category are healthy but have high potential viral-load exposure. This group includes medical personnel, caregivers of high-risk patients, people who use public transportation, first responders and other essential personnel who are crucial to the continued functioning of society. These patients should be encouraged to take prophylaxis against Covid-19 in accordance with the protocol noted below.
High Risk Patients
Patients are considered high risk if they are over the age of 45, or if they are younger than 45 but they have comorbidities, that is, they have other health conditions that put them at risk. These patients have between a 5 to 10% mortality rate if they are infected with Covid-19. These patients should be strongly encouraged to take prophylaxis against Covid-19 in accordance with the protocol noted below.
Protocol for Low Risk Patients:
Do nothing.
Completely optional:
Elemental Zinc 25mg 1 time a day
Vitamin D3 5000iu 1 time a day
Vitamin C 250-500mg 1 time a day
Quercetin 250mg 1 time a day or
Epigallocatechin-gallate (EGCG) 200mg 1 time a day
Protocol for Moderate / High Risk Patients:
Hydroxychloroquine (HCQ) 200mg once a day for 5 days, then HCQ 200-400mg
one time a week
Vitamin D3 5000 IU/day or 50000iu once a week
Vitamin C 1000mg once a day
Zinc 25-50mg/day
Or
Ivermectin 0.2 mg/kg - one dose on day 1 and day 3, then take one dose weekly
Vitamin D3 5000 IU/day or 50000iu once a week
Vitamin C 1000mg once a day
Quercetin 500mg/day
Zinc 25-50mg/day
The Indian Council of Medical Research (ICMR) adopted a recommendation [1] in favor of prophylactic hydroxychloroquine use for healthcare workers as early as March 23, 2020, which was then updated on May 22, 2020. Their proposed protocol recommended taking hydroxychloroquine 400mg twice a day on Day 1 followed by 400mg once a week, thereafter, however it did not include zinc.
Hydroxychloroquine has a very long half-life in the human body, and tends to concentrate its buildup in the lungs, making it highly protective in terms of preventing any breakthrough infections from becoming severe. However, it takes 6 weeks of weekly administration of hydroxychloroquine to build up the medication level to a steady state. In other words, protection against the SARS-CoV-2 virus is not fully optimized until 6 weeks after taking hydroxychloroquine once a week. This is the reason why Dr. Zelenko, contrary to the ICMR protocol, recommended taking hydroxychloroquine 200mg once a day for 5 days before taking it weekly, in order to shorten the window of suboptimal protection to approximately 4 weeks. A total intake of 2400mg of HCQ within a window of 40 days results in optimal protection, however it needs to be carefully distributed throughout the 40-day interval to avoid side effects, so there is a tradeoff between how fast you get to optimal protection versus chances of some side effects.
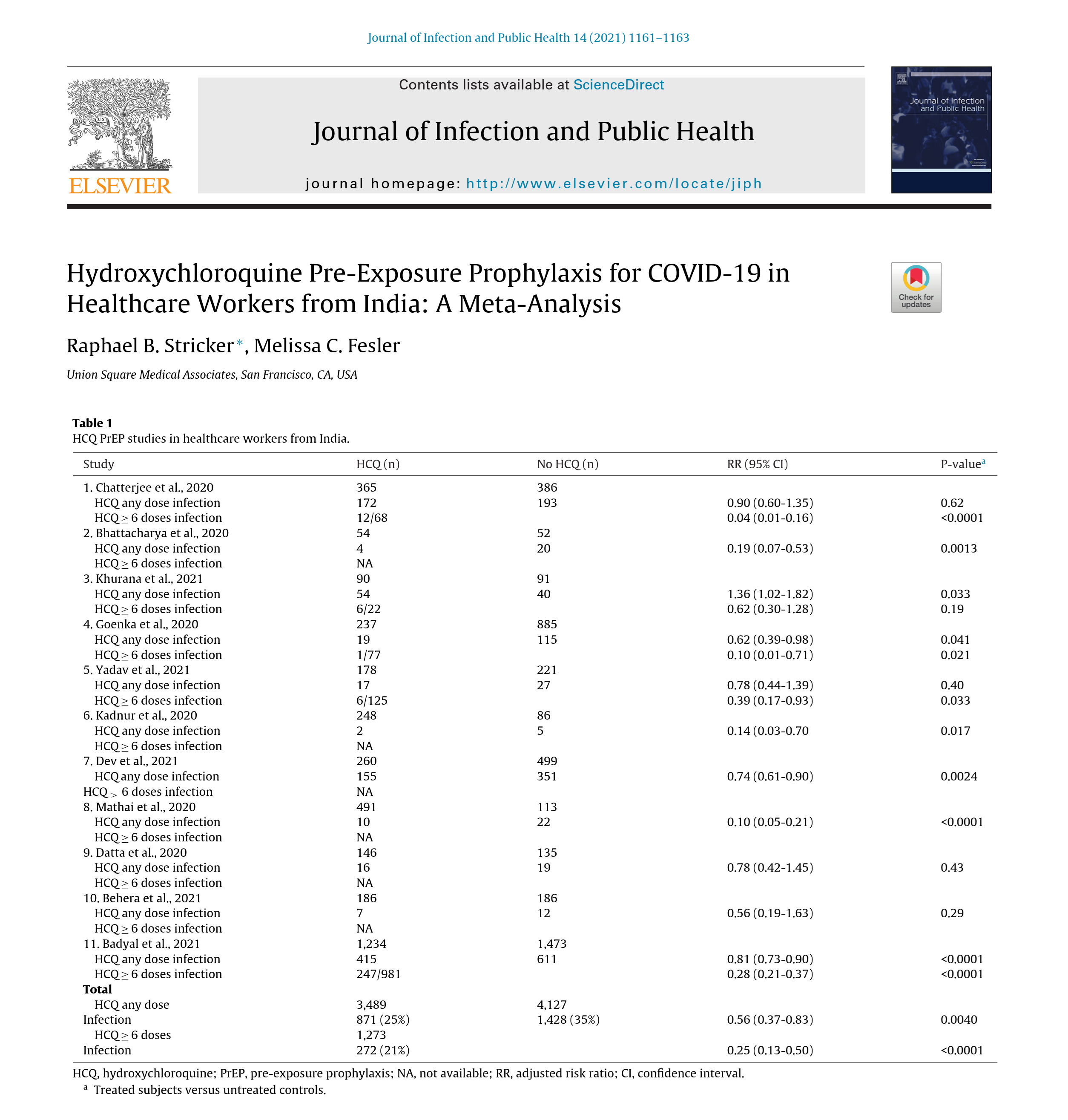
In the video presentation above, Dr. Raphael Stricker presented his landmark paper [2] on hydroxychloroquine pre-exposure prophylaxis, in which the following results of a meta-analysis of 11 cohort studies of Indian health-care workers using the ICMR prophylactic protocol was reported:
"In the 11 studies that included HCWs who used any HCQ PrEP, the infection rate was significantly decreased (RR 0.56, p = 0.0040). In the five studies that included HCWs who took at least six doses of weekly HCQ PrEP, the infection rate was reduced even further (RR 0.25, p < 0.0001). The uniform ICMR treatment protocol used in these studies argues against bias related to variations in dosing of HCQ."
RR is an abbreviation for "risk ratio" and, for example, RR 0.25 corresponds to preventing 3 out of 4 infections. In connection with these results, we can make the following observations:
1. The studies used in the meta-analysis involved healthcare workers who had substantially more exposure to increased viral loads relative to the general population. Furthermore, there is no clear statement that zinc was used in these studies. Consequently, with the use of zinc and for the general population we should expect an even better risk ratio.
2. There is a clear dose-response effect. Collectively, all 11 studies indicate a 44% reduction of infections. However, for the 5 studies in which the prophylactic protocol was used for at least 6 weeks, thus allowing hydroxychloroquine levels in the lungs to build up to full steady state, the reduction of infections was increased to 75%. This dose-response effect is additional evidence that prophylaxis does have a causal effect in preventing infections.
3. On basic mathematical modeling grounds, the actual risk ratio for symptomatic infection rate reduction is expected to be dependent also on the average initial viral load exposure for the cohort as well as the replication rate of the particular viral strains.
4. Being on prophylaxis is equivalent to initiating treatment from Day 0 and provides a much wider window of opportunity to diagnose and treat COVID-19, that is maximizing the odds of preventing hospitalizations and deaths. With prophylaxis, any breakthrough infections thus become opportunities to develop robust natural immunity, as safely as possible, by combining prophylaxis with early treatment using the McCullough protocol [3] for further protection against future exposures to the SARS-CoV-2 virus.
5. Evidence of the existence of some efficacy for the original triple-drug Zelenko protocol [4,5], implies the existence of some efficacy for the prophylactic protocol, with respect to reducing hospitalizations and deaths, in case of any symptomatic breakthrough infections. The reason for that is that 6 weeks of HCQ prophylaxis builds up the same HCQ levels in the lungs as 5 days of the higher therapeutic dosage by the Zelenko triple drug protocol. The difference is that after 6 weeks of prophylaxis you are locked and loaded from Day 0, and can then bring in the rest of the McCullough protocol [3] to handle the symptomatic infection.
Using chemoprophylaxis in conjunction with early treatment protocols was the optimal approach for navigating through the COVID-19 pandemic by minimizing hospitalizations and deaths to the maximum extent possible. We never had to "wait for a vaccine". We could have used prophylactic hydroxychloroquine to protect our high-risk population as early as April 2020, as was advocated by Dr. Zelenko, in conjunction with early outpatient treatment, using his Zelenko protocol, and later the McCullough protocol.
Download slides
ICMR prophylactic protocol
Zelenko's prophylactic protocol
References
[1] Indian Council of Medical Research, "Revised advisory on the use of Hydroxychloroquine (HCQ) as prophylaxis for SARS-CoV-2 infection (in supersession of previous advisory dated 23rd March, 2020)", 2020. Available at https://www.icmr.gov.in/pdf/covid/techdoc/V5_Revised_advisory_on_the_use_of_HCQ_SARS_CoV2_infection.pdf (accessed on January 9, 2024)
[2] R.B. Stricker and M.C. Fesler. "Hydroxychloroquine Pre-Exposure Prophylaxis for COVID-19 in Healthcare Workers from India: A Meta-Analysis", Journal of Infection and Public Health 14 (2021), 1161-1163
[3] P.A. McCullough, P.E. Alexander, R. Armstrong, C. Arvinte, A.F. Bain, R.P. Bartlett, R.L. Berkowitz, A.C. Berry, T.J. Borody, J.H. Brewer, A.M. Brufsky, T. Clarke, R. Derwand, A. Eck, J. Eck, R.A. Eisner, G.C. Fareed, A. Farella, S.N.S. Fonseca, C.E. Geyer, Jr., R.S. Gonnering, K.E. Graves, K.B.V. Gross, S. Hazan, K.S. Held, H. Thomas Hight, S. Immanuel, M.M. Jacobs, J.A. Ladapo, L.H. Lee, J. Littell, I. Lozano, H.S. Mangat, B. Marble, J.E. McKinnon, L.D. Merritt, J.M. Orient, R. Oskoui, D.C. Pompan, B.C. Procter, C. Prodromos, J.C. Rajter, J-J. Rajter, C. V.S. Ram, S.S. Rios, H.A. Risch, M.J.A. Robb, M. Rutherford, M. Scholz, M.M. Singleton, J.A. Tumlin, B.M. Tyson, R.G. Urso, K. Victory, E.L. Vliet, C.M. Wax, A.G. Wolkoff, V. Wooll, V. Zelenko. "Multifaceted highly targeted sequential multidrug treatment of early ambulatory high-risk SARS-CoV-2 infection (COVID-19)", Reviews in Cardiovascular Medicine 21 (4) (2020), 517-530
[4] R. Derwand, M. Scholz, V. Zelenko. "COVID-19 outpatients - early risk-stratified treatment with zinc plus low dose hydroxychloroquine and azithromycin: a retrospective case series study", International Journal of Antimicrobial Agents 56 (2020), 106214
[5] E. Gkioulekas, P.A. McCullough, V. Zelenko: "Statistical analysis methods applied to early outpatient COVID-19 treatment case series data", COVID 2(8) (2022), 1139-1182



Presentation: Hydroxychloroquine Pre-Exposure Prophylaxis for COVID-19 in Healthcare Workers from India: A Meta-Analysis